

The Lockdown regime, ushered in by the UK government on March 23rd and enacted into Law on March 25th, appears to have led to the premature deaths of tens of thousands of people in the UK. In my previous post LOKIN-20 The Lockdown Regime Causes Increasing Health Concerns we discussed the likelihood that the Lockdown would cause significant excess mortality.
With the release of the latest report on non COVID 19 related deaths from the Office of National Statistics we can now start to see the scale of those deaths.
The ONS reveal that between March 7th and May 1st (ONS Week 11–18) there were 46,380 excess death, over and above the statistical 5 year average, registered in England and Wales. Figures for Scotland and Northern Ireland are not included.
Of the 46,380 excess deaths 12,900 (27.8% of additional excess deaths) were not attributable to COVID 19. This suggests that 33,480 (72.2% of additional excess deaths) were attributable to COVID 19.
However, as we discussed in COVID 19 is a Statistical Nonsense it is by no means clear how many of those deaths were as a direct or even indirect result of COVID 19. The problem is that the UK State has created a system for registering COVID 19 deaths which is unusually vague, for the UK, and wide open both to error and misinterpretation.
All nations have their own registration processes and data collection systems, but the situation in the UK is not dissimilar to that in Italy. The Italian government imposed their severe lockdown on March 9th.
On March 20th, as significant numbers of assumed COVID 19 deaths mounted, Italy’s National Institute of Health (ISS) issued a report into the characteristics of the decedents.
Citing the research, which found no clear COVID 19 cause of death in 88% of deaths attributed to coronavirus, the scientific adviser to Italy’s minister of health, Professor Walter Ricciardi, said:
The way in which we code deaths in our country is very generous in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus……On re-evaluation by the National Institute of Health, only 12 per cent of death certificates have shown a direct causality from coronavirus.”
We might consider this in light of the statement made by Professor Ricciardi’s UK counterpart. Speaking on April 16th the UK’s Chief Scientific Officer, Sir Patrick Vallance, stated:
It is worth remembering again that the ONS rates are people who’ve got COVID on their death certificates. It doesn’t mean they were necessarily infected because many of them haven’t been tested. So we just need to understand the difference.”
The UK State instructed the ONS to record any and all mentions of COVID 19 on the death certificate (MCCD) as COVID 19 mortality. Furthermore, the ONS were told to accept suggested COVID 19 mortality figures from the Care Quality Commission (CQC) even if COVID 19 was not mentioned on the MCCD.
This has left the collection and reporting of COVID 19 mortality in England and Wales in total disarray. Certainly the MSM’s reporting of those statistics, which has overwhelmingly been in support of the Lockdown regime, is as close to meaningless as it is possible to get without simply making them up.
Between March 7th and May 1st figures from the CQC played no part in the ONS mortality analysis. The CQC didn’t start submitting their data to the ONS until April 29th. I mention it here, not only to highlight how absurd the COVID 19 mortality statistics have become, but also because CQC figures will be important as we attempt to assess the true scale of LOKIN-20 deaths in the UK.
UNDIAGNOSED COVID 19
The ONS state:
It is possible that symptoms may not be apparent or that COVID-19 could be mistaken for illnesses with similar symptoms. Some death certificates state that more information will be provided later, and some of these have since been updated to mention COVID-19. This supports the theory that COVID-19 is under-diagnosed at present on death certificates.”
This is an illogical statement from the ONS. It does not support their claim that COVID 19 has been under-diagnosed.
If symptoms are not apparent there is no reason to suspect that COVID19 was the cause of death. Presumably, nor were there any symptoms of rabies or malaria. You wouldn’t suspect they were a cause of death either, though you might if you followed ONS logic.
The ONS doesn’t tell us why MCCD’s have been updated later to mention COVID 19. Nor do we know how many of the non-COVID19 deaths were later changed to COVID 19 deaths.
The most reasonable explanation for this change is that the decedent passed away before test results were available or where a subsequent case note reviews indicated the presence of COVID19.
We will discuss positive test results later, but suffice to say they are a reason to reduce not increase claimed COVID19 mortality.
As previously discussed a case note review is by no means a reliable way to identify COVID 19. Not least of all for the fact that that the reviewing doctor may have never met the decedent. Elsewhere, in their report, the ONS state:
It is possible the conditions ‘other acute lower respiratory infections’ and ‘influenza and pneumonia’ could exhibit similar symptoms to COVID-19 and therefore be mistakenly recorded in place of COVID-19….it is possible that symptoms may not be apparent or that COVID-19 could be mistaken for illnesses with similar symptoms…”
This is an astute observation from the ONS. The symptoms of influenza, pneumonia and other acute respiratory infections are virtually indistinguishable from the most dangerous respiratory symptoms of COVID 19. While the ONS seem intent to suggest this means COVID 19 has been under-diagnosed, considerable over-diagnosis is far more plausible.
Prof Karol Sikora, former director of the World Health Organisation (WHO) cancer program, highlighted this concern recently. He stated that doctors appeared to be putting COVID 19 on to MCCD’s injudiciously with “any hint” of it’s presence being sufficient to record it as cause of death.
While he estimated that approximately half of the ONS reported COVID 19 deaths were attributable to COVID 19, it is perhaps a little unfair to blame the medical profession for this potentially excessive misdiagnosis.
Following the Coronavirus Act, the State, the NHS, the Royal College of Pathology and the ONS were among the many influential institutions who were compelled by the legislation to issue COVID 19 guidance to MCCD signing medical professionals. It practically guaranteed attribution of COVID 19 mortality on the flimsiest of evidence. For example, the ONS stated:
If before death the patient had symptoms typical of COVID 19 infection…it would be satisfactory to give ‘COVID-19’ as the cause of death.”
As the ONS acknowledges, these symptoms could have been caused by a range of respiratory illnesses. The obvious consequence of the guidance they issued is over, not under, diagnosis of COVID 19. Doctors have to follow policy like anyone else. They are not to blame for this problem. State legislators and policymakers are.
Seeing as COVID 19 is supposed to be a pandemic, if under diagnosis is an issue, we should see an unseasonable increase in pneumonia deaths within the non COVID19 mortality figures. Flu, COVID 19 and other similar respiratory illness often resolve as pneumonia in end stage palliative care.
Yet the ONS contradict this notion in their own report:
It unlikely that symptoms of COVID-19 have been mistaken for pneumonia since Week 14 (week ending 3 April 2020). It is possible this contributed to non-COVID-19 excess deaths observed before that time.”
The ONS report that the numbers of non COVID 19 deaths have been recalculated in order to provide the most up to date figures. The stated 12,900 figure is not evident in their released data sets for the Week 11–18 period.
There were no non-COVID 19 excess death in week 11. Between Week 12 to Week 18 there were 10,839 additional non-COVID19 deaths initially reported. Of these 421 (3.9%) occurred before Week 14. With misdiagnosed pneumonia being an unlikely reason for more than 96% of the reported non-COVID19 deaths, we must ask why the ONS would bother to suggest this may account for them.
Clearly, according to their own reported data analysis, it doesn’t. There is no basis for them to make such a claim.

[Click to enlarge]
ONS STRAWMEN
This theme of under diagnosed COVID 19 persist throughout their report without justification. The ONS note the significant increase in deaths from a range of conditions, recording significant spikes in deaths from asthma and diabetes within the non-COVID19 mortality statistics.
While they acknowledge that delayed care could be the cause, they also persist with their pet notion that COVID19 still might account for these deaths.
This could indicate that some people suffering from these conditions are not receiving care fast enough to prevent death occurring. It is also plausible that some of these deaths are because undiagnosed COVID-19 had exacerbated the pre-existing condition.”
For some reason the ONS also make a couple of strawman arguments to try to explain the non COVID 19 mortality. The first is reduced hospital capacity.
During the Lockdown regime hospital capacity increased. There was no reduction. While the ONS recognise that deaths have increasingly occurred at home and in care settings, rather than hospitals, their rationale to explain this seems odd.
They state both that the NHS has been adapted to deal with COVID 19 cases and that healthcare for non-COVID19 illness may have been reduced which may have increased mortality. With regard to reduced access to hospital treatment, the ONS state:
[This] could indicate that people who are very ill with these conditions are remaining at home when previously they may have been admitted to hospital or a hospice for near end-of-life care.”
This is true. However, their report is supposed to be an analysis of the 12,900 additional excess deaths that occurred in a 7 week period in England and Wales. Not only have the ONS framed this within the context of strawman argument, they appear to be suggesting that patients not being treated in hospital just happened. People simply remained at home, as if this were their choice.

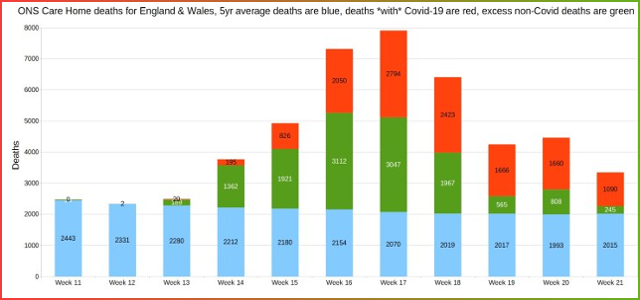
ONS statistics – Graphics from Christopher Bowyer [click to enlarge]
If that analysis seems odd, the ONS strawman explanation of death registration changes is downright bizarre. The argument they present is that the Coronavirus Act improved the efficiency of the registration process.
The ONS are in the business of reporting mortality statistics. For them, an improvement in the speed of the registration process is one measure of improved efficiency. However, if those registered death certificates provide increasingly meaningless causes of death, haste has significantly reduced efficiency.
Deaths are referred to coroners where the cause of death is not clear. This reduces the speed of registration but also improves accuracy, from a statistical perspective. The Coronavirus Act 2020 more or less ruled out any referral to a coroner. The UK’s chief coroner issued the following advice to coroners:
The aim of the system should be that every death from COVID-19 which does not in law require referral to the coroner should be dealt with via the MCCD process.”
Doctors were instructed to assume symptoms of respiratory illness indicated COVID 19. If they were uncertain, referral to a coroner was certainly a waste of time and the Coronavirus Act removed access to the second opinion of a Medical Examiner.
For some unfathomable reason, the ONS appear to agree that COVID 19 is a uniquely clear cause of death. Despite the fact that they recognise COVID 19 symptoms are more or less the same as those of numerous other infections, a diagnosis of COVID 19 somehow removes any doubt. The Coronavirus Act has made sure of this and the ONS believe this is more efficient:
This would increase efficiency in registering cases that would have typically gone to inquest.”
Troubling inquests and corroborating medical opinions, to ensure the stated cause of death is accurate, are unnecessary for all COVID 19 deaths. Though what this has to do with non-COVID19 deaths is anyone’s guess. Not much, according to the ONS, who state:
This suggests that despite observing efficiency improvements in registrations, these improvements themselves are unlikely to be driving much of the increase in death registrations observed in recent weeks.”
Not only does this raise significant concerns about the accuracy of the ONS reported statistics, it begs the question why they felt the need to include a suggested explanation, in their written analysis of non COVID 19 deaths, if they had already ruled it out.
This appears to have been included to promote the idea that the Coronavirus Act improved registration efficiency.
Yet, within their own report, the ONS provide more than sufficient reason to seriously question that claimed efficiency gain. The Coronavirus Act reduced the accuracy and reliability of mortality statistics in England and Wales. That this doesn’t seem to matter to the ONS is worrying.
EVIDENCE OF LOCKDOWN REGIME DEATHS
It is apparent that the Lockdown regime has caused significant loss of life. There is no doubt that delayed treatment for serious conditions increases the mortality risk considerably.
At the time of writing (10/06/2020) COVID 19 is said to have affected 0.4% of the UK populations and 0.06% have reportedly died as a result.
Cancer alone kills 0.24% of the population every year in the UK. Even if you accept that all claimed deaths from COVID 19 were as a result of the syndrome, cancer kills at least four times as many people.
In 2018 541,589 people died in England and Wales. This represents 0.92% of the population which means approximately 0.15% of the population die every two months. The top 5 leading causes of death account for more than 40% of those deaths.
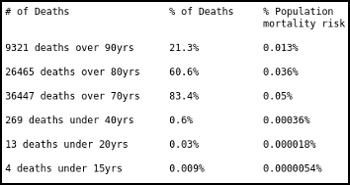
On average these five causes kill 0.37% of the population every year, equating to approximately 0.06% every two months. Roughly the same figure as reported COVID 19 deaths. Yet for these people, during the Lockdown regime, treatment and essential screening has effectively been withheld.
During the same period hospital bed occupancy has been at an all time low. Additional capacity was added in the form of the various Nightingale hospitals, though these have not been required to treat COVID 19 patents.
During the Lockdown regime, cancer screening and treatment was put on hold. Cancer Research UK estimate that 290,000 people have missed cancer follow ups, indicating that around 20,000 current cancer sufferers, who would otherwise have been detected, remain without a diagnosis in the UK.
They state that 2.1 million people have missed screening appointment, potentially at the cost of another 3,800 lives. The impact upon cancer survival rates alone has been devastating.
In London the mean ambulance response time increased by 43 minutes. Nationally the average ambulance response times for the most serious category 1 emergencies rose to 8 minutes 7 seconds, 1 minute and 7 seconds above the recommended maximum.
Jason Oke from the Nuffield Department of Primary Care Health Sciences at the Oxford University reported that in May both general A&E presentations and those for heart attacks were down by half. Cardiovascular disease kills nearly 170,000 people every year in the UK.
With an average mortality of 460 deaths per day, a 50% drop in presentations, over the nearly three months long Lockdown regime period, has and will significantly increase mortality from cardiovascular disease.
Crucial surgery and diagnostic tests, for a range of other serious conditions, have been delayed in huge numbers. As the NHS confederation warns that waiting lists will exceed 10 million, the mainstream media insist that you believe this is due to coronavirus.
The best you can say about this claim is that it is doubtful. We should not discard the possibility that it is intentionally deceptive.
With more than enough capacity to treat both the seriously ill non-COVID19 and COVID19 patients, there is no doubt that the Lockdown regime has resulted in the unnecessary deaths of at least 12,900 people. Unfortunately, further analysis of the COVID19 statistics suggests the figure is much higher.
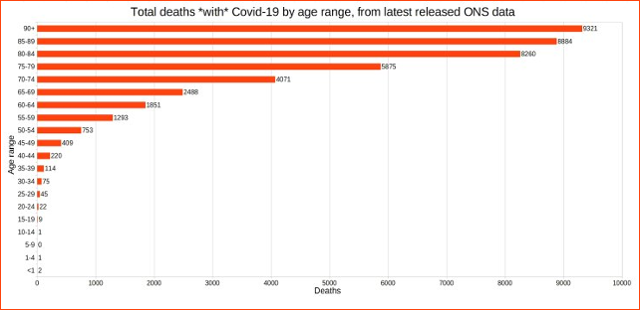
ONS statistics – Graphics from Christopher Bowyer
THE REAL SCALE OF LOKIN 20 MORTALITY.
If the denial of healthcare were an identifiable syndrome we could perhaps call it LOKIN 20. In order to assess the impact of LOKIN-20 we need to consider the excess mortality that we would not otherwise expect to occur. It is this additional excess mortality, attributed to COVID 19, the MSM commonly report in their daily coronavirus updates.
Taken form a variety of sources, on the May 9th 2020 the BBC reported that these excess deaths stood at 63,708 in the UK. This reported mortality includes notifications of suspected COVID 19 deaths from the Care Quality Commission (CQC). An unknown number of these may not even record COVID 19 on the MCCD.
Public Health England did not not record any statistically significant excess mortality in England until Week 13 (week ending 1st April). Therefore the reported 63,708 excess deaths have occurred entirely during the Lockdown regime period, up to June 9th.
Using ONS data for England and Wales we can calculate an estimate of the likely percentage of deaths that were genuinely attributable to COVID 19. We can then apply these percentages to the figures reported by the BBC to extrapolate estimates for the UK.

Unless there is some unknown pathogen ravaging the nation, what remains are excess deaths which correspond precisely with the Lockdown regime period. We don’t have any other explanation for this loss of life, but all deaths occurred during the Lockdown. We will call this LOKIN 20 mortality.
With 50,107 deaths allegedly attributed to COVID 19, the BBC report 13,601 LOKIN 20 deaths. Of the 50,107 COVID 19 deaths 9,510 were identified by symptoms alone. As previously discussed, it is not clear how many of these deaths can legitimately be attributed to COVID 19.
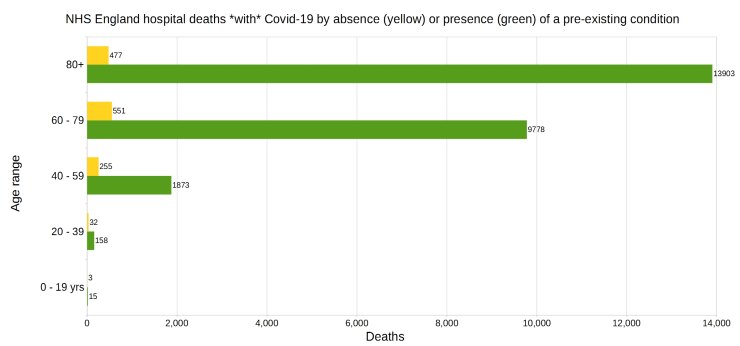
Approximately 95% of COVID 19 decedents have at least one other serious comorbidity. While this brings into question all of these claimed COVID 19 deaths, where diagnosis is by observation alone and both pneumonia & influenza are also mentioned on the death certificate, it is not reasonable to claim these deaths were from COVID 19.

For weeks 14 to 22 the ONS report that 37.3% of all COVID 19 deaths also mentioned both pneumonia and influenza. While we don’t know the distribution of these deaths between those identified by test results and those identified merely by symptom, we can reasonably state that at least 3,547 of the 9,510 symptom diagnosis were inconclusive. This leaves us with a potential LOKIN 20 mortality figure of 17,148.
The BBC state that 40,597 COVID 19 deaths were confirmed following positive tests results. There is a significant problem with claiming that a positive test result for SARS-CoV-2 proves that the patient was suffering from COVID 19.
A considerable number of people who test positive for SARS-CoV-2 are asymptomatic. This means they have the virus, not necessarily the resultant syndrome of COVID 19.
Without COVID 19 they don’t have a disease that will impact their health. Just because someone is critically ill with a heart condition, testing positive for SARS-CoV-2 doesn’t mean that COVID 19 is making their condition worse. Without the symptoms it almost certainly isn’t.
A study of asymptomatic SARS-CoV-2 patients in China found that the presence of the virus alone had little to no impact on their presenting conditions. Nearly 80% of the studied patients did not develop COVID 19, although CT scans possibly indicated signs of the disease.
The British Medical Journal report that Australian researchers thoroughly tested all the passengers on a quarantined cruise ship. Cruise ships are almost the perfect incubator for a viral infection. Studying COVID 19 in such an isolated population is of particular value.
Approximately 59% of the 217 passengers tested positive for SARS-CoV-2. This is in keeping with the estimates of the UK government’s chief scientific adviser, Sir Patrick Valance, who stated that COVID 19 herd immunity would be achieved with a 60% infection rate.
Again, 81% of those infected were asymptomatic. Asymptomatic rates on two quarantined aircraft carriers, the USS Theodore Roosevelt and the French Charles de Gaulle, were 58% and 48% respectively.
A similar figure of 78% asymptomatic infection was found in a study by Chinese researchers who tested overseas arrivals into their country. They showed no symptoms and therefore there was no evidence they were suffering the ill effects of COVID 19.
Another study of an isolated community of approximately 3000 people in the northern Italian village of Vo’Euganeo found similar results. Sergio Romagnani, professor of clinical immunology at the University of Florence, stated that between 50%-75% of positive test cases were asymptomatic.
Depending upon which study you look at this asymptomatic rate varies between 5% up to 80%. For our purpose, estimating the likely impact of the Lockdown regime, we’ll use the asymptomatic median of 42.5% of positive test cases.
This is lower than most study estimates but many of them are based on data models. We’ll stick to this conservative estimate in light of the empirical data measured in isolated communities.
This means that 17,211 of the claimed 40,497 COVID 19 deaths identified by SARS-CoV-2 positive test results are unlikely to have had COVID 19. Added to the potential 17,148 LOKIN 20 deaths already noted, it appears LOKIN 20 accounts for at least 34,359 of the 63,708 deaths reported by the BBC.
Graphics from Christopher Bowyer
[click to enlarge]
Apparently the Lockdown regime has already led to the premature deaths of at least 54% of the people the State and the MSM report as dying from the direct or indirect impacts of coronavirus. This is slightly more than the 50% estimate of Professor Karol Sikora.
Critics will rightly point out that I have made some assumptions to arrive at this figure. For example, we don’t know how many of those diagnosed by symptoms alone actually had COVID 19, nor how many positive tests for SARS-CoV-2 were either accurate or led to the patient developing COVID 19. In truth, we may never know.
However the UK State’s Lockdown Regime, despite claims of being led by the science, is based upon the computer models of Imperial College. These were not only wildly speculative, they were also demonstrably wrong.
The calculation presented here is based upon the cited empirical scientific evidence. Given that the Italian National Institute of Health (ISS) found that only 12% of claimed COVID 19 deaths could be clearly attributed to the disease, I have erred on the side of caution. 34,359 LOKIN 20 deaths is a conservative estimate.
Sadly, it appears the UK State are intent upon continuing with their Lockdown regime. In all likelihood this policy has already led to the premature deaths of more than 34,000 British people. Unfortunately that figure is set to increase.
The NHS are already faced with a staggering backlog of cases for critical health conditions other than COVID 19. It is difficult to see how further considerable mortality can be avoided. Worse still, the economic impact of the Lockdown regime is disastrous. Every day that it continues the situation deteriorates.
The UK Gross Domestic Product (GDP) fell by a jaw dropping 20.4% in April. To put this into context, the sharpest monthly drop of GDP following the 2008 financial crisis was 1%. April 2020’s decline is more than nine times greater the pre-Lockdown regime record of 2.2%, set in June 2002.
Whereas COVID19 has no statistically significant impact upon child mortality, the poverty wrought by the Lockdown regime certainly will.
The words of George Batchelor, a co-founder of Edge Health, who provide data analysis to the NHS, are disquieting.
Predicting that health services will be overwhelmed by the backlog, and the other impacts of the Lockdown regime, he stated:
If projected forwards, these numbers get so large it is hard to relate to them on a personal level.”
We can only hope that Edge Health’s warnings are overly pessimistic. However, it is clear that any large second or third wave of mortality will be blamed upon coronavirus, either directly or as a suggested consequence, by the State and the mainstream media.
That will be a deception. The Lockdown regime is the cause and the health costs of LOKIN 20 are the result. I hope those of you who read this, who find the logic presented reasonable, will reject those claims when they arrive. More importantly, please tell others why.
By Iain Davis
Originally published by Off-Guardian.org
The 21st Century
The views expressed in this article are solely those of the author and do not necessarily reflect the opinions of 21cir.