

Closing down the Global Economy as a means to combating the Virus. That’s what they want us to believe. If the public had been informed that Covid-19 is “similar to Influenza”, the fear campaign would have fallen flat…
The data and concepts have been manipulated with a view to sustaining the fear campaign.
The estimates are meaningless. The figures have been hyped to justify the lockdown and the closure of the national economy, with devastating economic and social consequences. The Virus is held responsible for poverty and mass unemployment.
Confirmed by prominent scientists as well as by official public health bodies including the World Health Organization (WHO) and the US Center for Disease Control and Prevention (CDC). Covid-19 is a public health concern but it is NOT a dangerous virus.
The COVID-19 crisis is marked by a public health “emergency” under WHO auspices which is being used as a pretext and a justification to trigger a Worldwide process of economic, social and political restructuring. Social engineering is being applied. Governments are pressured into extending the lockdown, despite its devastating economic and social consequences.
There is no scientific basis for implementing the closing down of the global economy as a means to resolving a public health crisis.
Both the media and the governments are involved in spreading disinformation.
The fear campaign has no scientific basis.
Our objective is to reassure people Worldwide. Your governments are LYING. In fact they are lying to themselves.
We start by defining the virus and the tests which are being used to “identify the virus”.
1 What is Covid-19, SARS-COV-2.
Below is the official WHO definition of Covid-19:
Coronaviruses are a large family of viruses which may cause illness in animals or humans. In humans, several coronaviruses are known to cause respiratory infections ranging from the common cold to more severe diseases such as Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS). The most recently discovered coronavirus causes coronavirus disease COVID-19.
The most common symptoms of COVID-19 are fever, dry cough, and tiredness. … These symptoms are usually mild and begin gradually. Some people become infected but only have very mild symptoms. Most people (about 80%) recover from the disease without needing hospital treatment. Around 1 out of every 5 people who gets COVID-19 becomes seriously ill and develops difficulty breathing.
“COVID-19 is similar to SARS-1″: According to Dr. Wolfgang Wodarg, pneumonia is “regularly caused or accompanied by corona viruses”. Immunologists broadly confirm the CDC definition. COVID-19 has similar features to a seasonal influenza coupled with pneumonia.
According to Anthony Fauci (Head of NIAID), H. Clifford Lane and Robert R. Redfield (Head of CDC) in the New England Journal of Medicine
…the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.
Dr. Anthony Fauci is lying to himself. In his public statements he says that Covid is “Ten Times Worse than Seasonal Flu”.
He refutes his peer reviewed report quoted above. From the outset, Fauci has been instrumental in waging the fear and panic campaign across America:


Screenshot The Hill, March 19, 2020
Covid-19 versus Influenza (Flu) Virus A and Virus B (and subtypes) (Bear in mind seasonal influenza is not a coronavirus)
Rarely mentioned by the media or the governments, The CDC confirms that Covid-19 is similar to Influenza
“Influenza (Flu) and COVID-19 are both contagious respiratory illnesses, but they are caused by different viruses. COVID-19 is caused by infection with a new coronavirus (called SARS-CoV-2) and flu is caused by infection with influenza viruses. Because some of the symptoms of flu and COVID-19 are similar, it may be hard to tell the difference between them based on symptoms alone, and testing may be needed to help confirm a diagnosis. Flu and COVID-19 share many characteristics, but there are some key differences between the two.”
If the public had been informed and reassured that Covid is “similar to Influenza”, the fear campaign would have fallen flat.
The lockdown and closure of the national economy would have been rejected outright.
2. The Test for Covid-19 “Confirmed Cases”
The standard Covid test is the Reverse transcription polymerase chain reaction (RT-PCR):
“The COVID-19 RT-PCR test is a real-time reverse transcription polymerase chain reaction (rRT-PCR) test for the qualitative detection of nucleic acid from SARS-CoV-2 in upper and lower respiratory specimens … collected from individuals suspected of COVID 19 … [as well as] from individuals without symptoms or other reasons to suspect COVID-19 infection. …
This test is also for use with individual nasal swab specimens that are self-collected using the Pixel by LabCorp COVID-19 test home collection kit … The COVID-19 RT-PCR test is also for the qualitative detection of nucleic acid from the SARS-CoV-2 in pooled samples, using a matrix pooling strategy (FDA, LabCorp Laboratory Test Number: 139900)
First, it should be understood that the Covid-19 RT-PCR Test is similar to that used in relation to Influenza. This test is based on upper and lower respiratory specimens.
The criteria and guidelines confirmed by the CDC pertaining to “The CDC 2019-Novel Coronavirus (2019-nCoV) Diagnostic Panel” are as follows (Read carefully):
Results are for the identification of 2019-nCoV RNA. The 2019-nCoV RNA is generally detectable in upper and lower respiratory specimens during infection. Positive results are indicative of active infection with 2019-nCoV but do not rule out bacterial infection or co-infection with other viruses. The agent detected may not be the definite cause of disease. Laboratories within the United States and its territories are required to report all positive results to the appropriate public health authorities.
Negative results do not preclude 2019-nCoV infection and should not be used as the sole basis for treatment or other patient management decisions. Negative results must be combined with clinical observations, patient history, and epidemiological information.
What this suggests is that a positive infection could be the result of other viruses as well as other corona viruses as well as viruses related to seasonal influenza (e.g. Viruses A, B, C, D).
And, according to the CDC it “does not rule out “bacterial infection or co-infection with other viruses. The agent detected may not be the definite cause of disease.” (CDC)
The following diagram summarizes the process of identifying positive and negative cases: All that is required is the presence of “viral genetic material” for it to be categorized as “positive”. The procedure does not identity or isolate Covid-19. What appears in the tests are fragments of the virus
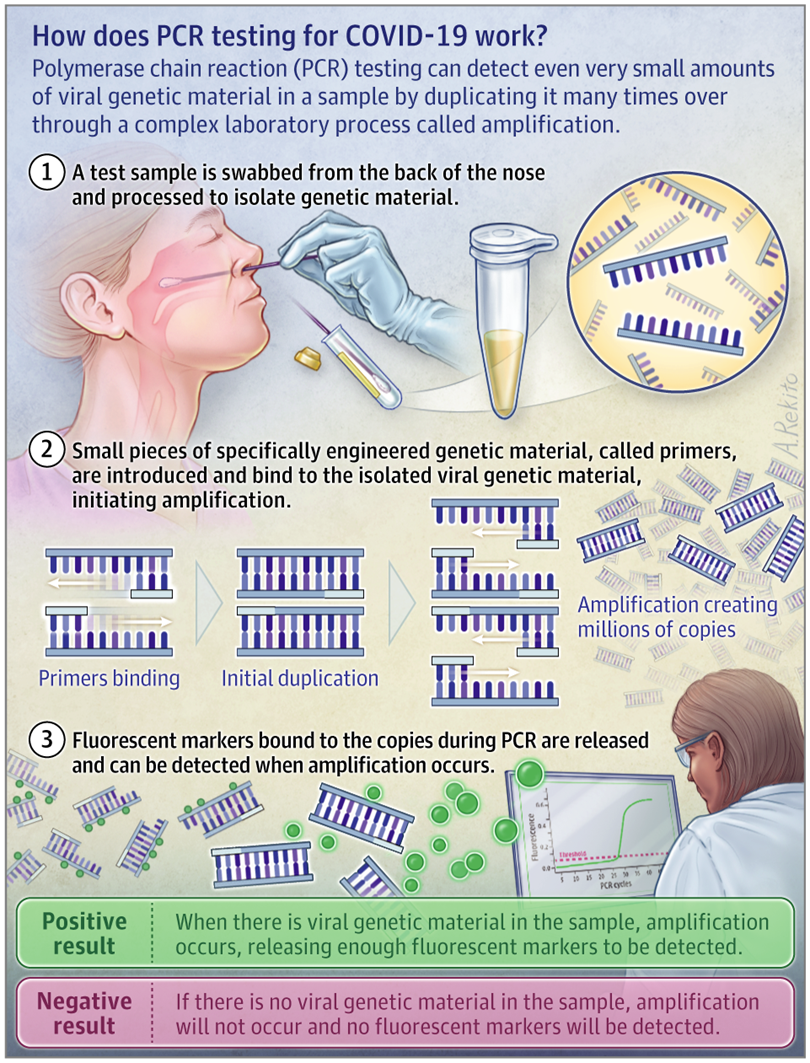
While SARS-CoV-2 –namely the the virus which is said to cause COVID-19 (erroneously categorized as a disease rather than a virus), was isolated in a laboratory test in January 2020, the RT-PCR test does not identify/detect the Covid-19 virus. What it detects are fragments of several viruses. According to renowned Swiss immunologist Dr B. Stadler
So if we do a PCR corona test on an immune person, it is not a virus that is detected, but a small shattered part of the viral genome. The test comes back positive for as long as there are tiny shattered parts of the virus left. Even if the infectious viri are long dead, a corona test can come back positive, because the PCR method multiplies even a tiny fraction of the viral genetic material enough [to be detected].
Bear in mind: Because the RT-PCR test is similar to the test used in the case of influenza (flu) (eg viruses A,B), a positive test does not mean that you test positive for Covid-19.
The Question is Positive for What?? The PCR does not detect the identity of the virus, According to Dr. Pascal Sacré,
these tests detect viral particles, genetic sequences, not the whole virus.
In an attempt to quantify the viral load, these sequences are then amplified several times through numerous complex steps that are subject to errors, sterility errors and contamination
Positive RT-PCR is not synonymous with COVID-19 disease! PCR specialists make it clear that a test must always be compared with the clinical record of the patient being tested, with the patient’s state of health to confirm its value [reliability]
The media frighten everyone with new positive PCR tests, without any nuance or context, wrongly assimilating this information with a second wave of COVID-19.
Presumptive vs. Confirmed Cases
In the US, the CDC data include both “confirmed” and “presumptive” positive cases of COVID-19 reported to CDC or tested at CDC since January 21, 2020″.
The presumptive positive data does not confirm coronavirus infection: Presumptive testing involves “chemical analysis of a sample that establishes the possibility that a substance is present“ (emphasis added). The presumptive test must then be sent for confirmation to an accredited government health lab. (For further details see: Michel Chossudovsky, Spinning Fear and Panic Across America. Analysis of COVID-19 Data, March 20, 2020)
Similarly in Canada, “A point-of-care test” is a “rapid test done at the time and place of care, such as a hospital or doctor’s office”. It consists in collecting “samples from the nose or throat using swabs”, which are then tested on site, with almost immediate results (in 30 to 60 minutes). But it does not confirm the presence of COVID-19.
Serological testing or Antibody Tests for COVID-19
According to the CDC, Serological tests do not detect the virus itself, “they detect the antibodies produced in response to an infection.” Serological tests are not used for “early diagnosis of COVID-19.”
How is the COVID-19 Data Tabulated?
Below is a screen shot of the CDC form entitled Human Infection with 2019 Novel Coronavirus Case Report Form to be filled in by authorized medical/ health personnel
Note the categorization of probable cases, bearing in mind that the lab confirmed case is misleading. No way to identify the covi-19 virus in a PCR lab test
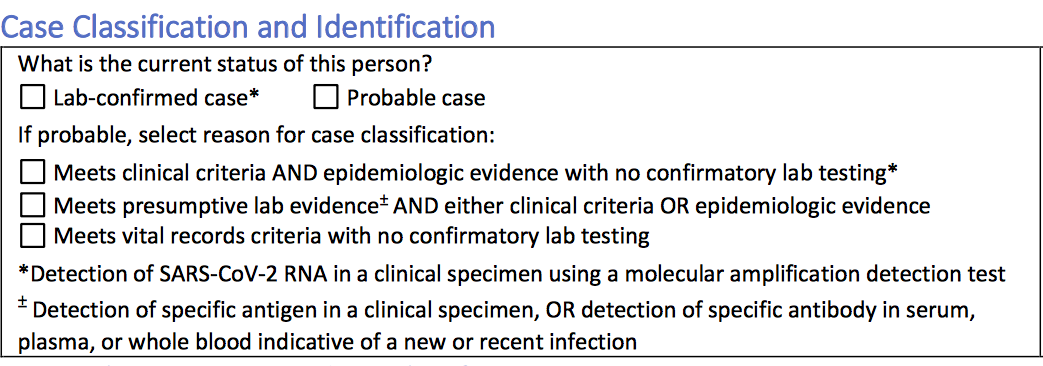
In the US, the probable (PC) and the lab confirmed cases (CC) are lumped together. And the total number (PC + CC ) constitutes the basis for establishing the data for COVID-19 infection. It’s like adding apples and oranges.
The total figure (PC+CC) categorized as “Total cases” is meaningless. It does not measure positive COVID-19 Infection.
Most of the presumptive tests are undertaken by private clinics or commercial clinics.
In the UK, according to a Daily Telegraph May 21 report: “samples taken from the same patient are being recorded as two separate tests in the Government’s official figures”.
This is only one example of data manipulation. In the US, clinics are paid ($$$) to hike up the number of Covid-19 admissions. A probable case does not require a lab exam: “Meets vital records criteria with no confirmatory lab testing” (see form above)
COVID-19 Recovery Rates
The CDC Data tabulates both “confirmed” and “presumptive” positive cases since January 21, 2020. Yet what it fails to make public is that among the confirmed and presumptive cases, a large number of Americans have recovered. But nobody talks about recovery. It does not make the headlines.
Falsification of Death Certificates
At the outset of the pandemic, the CDC had been instructed to change the methodology regarding Death Certificates with a view to artificially inflating the numbers of “Covid deaths”. According to H. Ealy, M. McEvoy et al
“The 2003 guidelines for establishing death certificates had been cancelled. “Had the CDC used its industry standard, Medical Examiners’ and Coroners’ Handbook on Death Registration and Fetal Death Reporting Revision 2003, as it has for all other causes of death for the last 17 years, the COVID-19 fatality count would be approximately 90.2% lower than it currently is.” (Covid-19: Questionable Policies, Manipulated Rules of Data Collection and Reporting. Is It Safe for Students to Return to School? By , August 09, 2020
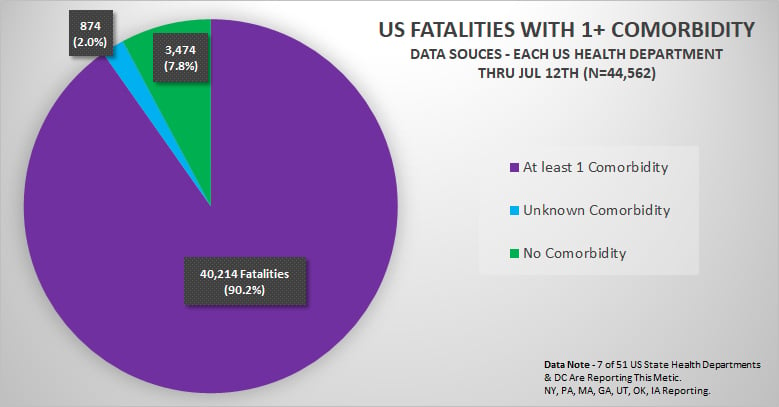
CDC Deaths Attributed to COVI-19. Comorbidities
The latest CDC report confirms that 94% of the deaths attributed to Covid have “comorbidities”,(i.e. deaths dues other causes).
For 6% of the deaths, COVID-19 was the only cause mentioned. For deaths with conditions or causes in addition to COVID-19, on average, there were 2.6 additional conditions or causes per death. The number of deaths with each condition or cause is shown for all deaths and by age groups.
On March 21, 2020 the following specific guidelines were introduced by the CDC regarding Death Certificates (and their tabulation in the National Vital Statistics System (NVSS)
COVID-19: The “underlying cause of death”
Will COVID-19 be the underlying cause of death? This concept is fundamental. The underlying cause of death is defined by the WHO as “the disease or injury that initiated the train of events leading directly to death”.
What the CDC is recommending with regards to statistical coding and categorization is that COVID-19 is expected to be the underlying cause of death “more often than not.”
“What Happens if Certifiers Report Terms other than the Suggested Term?”(see below)
The Certifier is not allowed to report coronavirus without identifying a specific strain. And the guideline recommends that COVID-19 be indicated, when in fact the nature of the PCR test does not isolate the Covid-19 virus. (2019 coronavirus strain).
(see below): (source CDC)
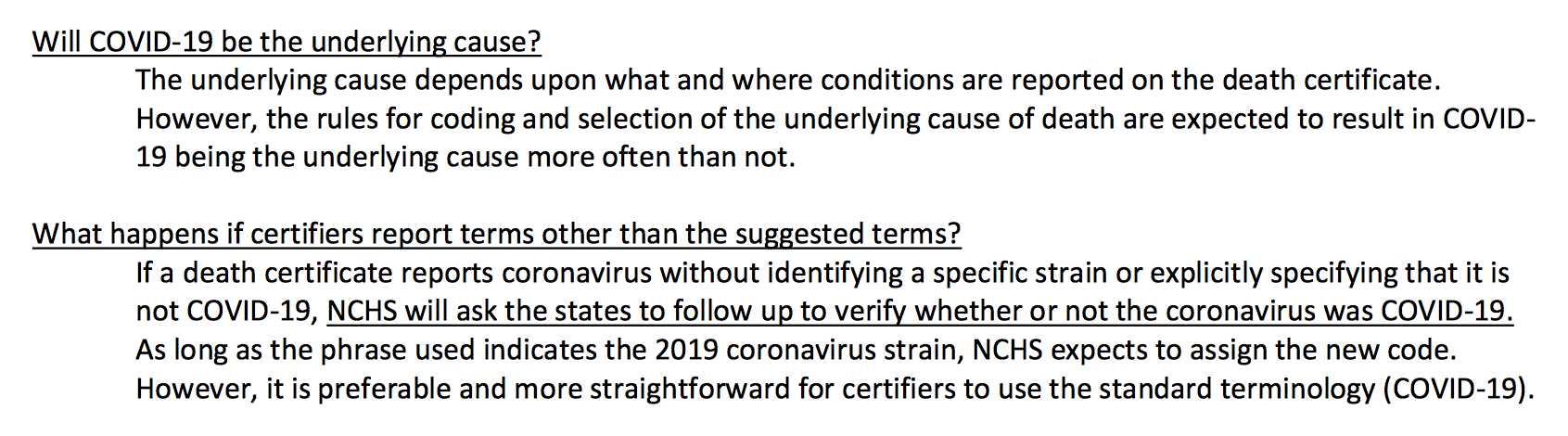
Will COVID-19 be the underlying cause of death?
“The underlying cause depends upon what and where conditions are reported on the death certificate. However, the rules for coding and selection of the underlying cause of death are expected to result in COVID- 19 being the underlying cause more often than not.
What happens if certifiers report terms other than the suggested terms?
If a death certificate reports coronavirus without identifying a specific strain or explicitly specifying that it is not COVID-19, NCHS will ask the states to follow up to verify whether or not the coronavirus was COVID-19.
As long as the phrase used indicates the 2019 coronavirus strain, NCHS expects to assign the new code. However, it is preferable and more straightforward for certifiers to use the standard terminology (COVID-19).
What happens if the terms reported on the death certificate indicate uncertainty?
If the death certificate reports terms such as “probable COVID-19” or “likely COVID-19,” these terms would be assigned the new ICD code. It Is not likely that NCHS will follow up on these cases.
If “pending COVID-19 testing” is reported on the death certificate, this would be considered a pending record. In this scenario, NCHS would expect to receive an updated record, since the code will likely result in R99. In this case, NCHS will ask the states to follow up to verify if test results confirmed that the decedent had COVID- 19.
… COVID-19 should be reported on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death. Certifiers should include as much detail as possible based on their knowledge of the case, medical records, laboratory testing, etc.”
These specific guidelines have indelibly contributed to increasing Covid-19 as the recorded “cause of death”
And this despite the fact that the relevant lab texts (i.e. RT PCR) provide misleading results. Bear in mind that a Covid-19 cause of death does not require a lab exam.
Video
Summary
- Covid-19 is Similar to Influenza
- The whole exercise of PCR testing and establishing data of Covid-19 infection is flawed.
- The figures are fabricated and so are the death certificates.
- “Confirmed Cases” are not confirmed.
- The RT-PCR Test Does not isolate the Covid-19 virus.
These inflated Covid positive “estimates” (from the PCR test) are then used to sustain the fear campaign. The hype in Covid-19 deaths is based on flawed and biased criteria.
Governments are currently involved in increasing the number of PCR tests with a view to inflating the number of so-called Covid-19 positive cases.
The RT- PCR tests do not prove anything:
“Today, as authorities test more people, there are bound to be more positive RT-PCR tests. This does not mean that COVID-19 is coming back, or that the epidemic is moving in waves. There are more people being tested, that’s all.”
This procedure of massive data collection is there to provide supportive (fake) “estimates” to justify the so-called Second Wave.
The Endgame is to maintain the economic lockdown, enforce the compulsory wearing of the face mask, social distancing including the closure of schools, colleges and universities.
The tendency is towards a police state. It is all based on a Big Lie.
We need a mass movement, nationally and internationally to reverse the tide.
Mass demonstrations barely reported by the corporate media have taken place in major European capitals including London, Dublin and Berlin.
Corrupt politicians in high office must be (peacefully) removed.
Revealing the lies and deceptions is the first priority. Dismantling the fear campaign. Reveal the media disinformation campaign.
National economies must be reopened…
***
By Prof Michel Chossudovsky
The original source of this article is Global Research
Copyright © Prof Michel Chossudovsky, Global Research, 2020
Republished by The 21st Century
The views expressed in this article are solely those of the author and do not necessarily reflect the opinions of 21cir.